Introduction
There is a particular kind of medical frustration that millions of people know intimately.
It is the persistent back pain that continues long after an injury has healed.
The exhaustion that cannot be explained by blood tests.
The dizziness, digestive problems, headaches, muscle tension, fatigue, or widespread pain that persist despite years of appointments, scans, treatments, and specialist visits.
Many people with these symptoms eventually arrive at the same uncomfortable place. Their symptoms are very real, but medicine struggles to explain them. Tests may come back normal or inconclusive. Findings on scans may not fully account for the severity of the symptoms. Treatments that make sense on paper often provide little lasting relief.
For decades, many patients in this situation heard some version of the same message:
“Everything looks normal.”
“It’s probably stress.”
“There is nothing seriously wrong.”
Even when offered with good intentions, those explanations often felt dismissive. Patients were left with the impression that medicine had run out of answers.
Yet there is an interesting contradiction at the heart of this story.
Medicine has understood for a very long time that the mind and body influence one another. Doctors have observed the effects of stress, fear, grief, anxiety, and emotional strain on physical health for centuries. The idea that thoughts and emotions can affect the body is not new. In fact, it is one of the oldest observations in medicine.
What is new is our growing understanding of how this happens.
Over the last several decades, advances in neuroscience, immunology, and pain research have begun to provide explanations that earlier generations of physicians simply did not have. These discoveries have given rise to a new family of approaches often referred to as neuroplastic, mind-body, or brain-based treatments.
Among the most widely discussed are approaches such as Pain Reprocessing Therapy (PRT), Emotional Awareness and Expression Therapy (EAET), and other interventions based on the idea that the nervous system can learn symptom patterns—and, under the right conditions, can also learn something new.
Despite growing evidence, these approaches remain controversial in some circles.
To understand why, it helps to understand the long road that led here.
This is not the story of one medical model replacing another.
It is the story of an idea evolving over more than a century as science gradually caught up with what many clinicians had been observing all along.
A Note on Scientific Humility
Before exploring that history, an important clarification is necessary.
This article is not arguing that all chronic symptoms are neuroplastic.
It is not suggesting that medical evaluation should be skipped.
It is not claiming that structural disease, injury, inflammation, infection, or genetics do not matter.
They do.
A broken bone remains a broken bone.
Cancer remains cancer.
Autoimmune diseases remain autoimmune diseases.
The goal of this article is not to replace conventional medicine with a different belief system.
Rather, it is to explore how scientific understanding of the relationship between the brain, body, and symptoms has evolved over time—and why some emerging approaches remain controversial despite growing evidence.
As with most things in medicine, reality is usually more complex than any single explanation.
Part I: The Origins of Psychosomatic Medicine
The word psychosomatic comes from two Greek words:
- Psyche, meaning mind
- Soma, meaning body
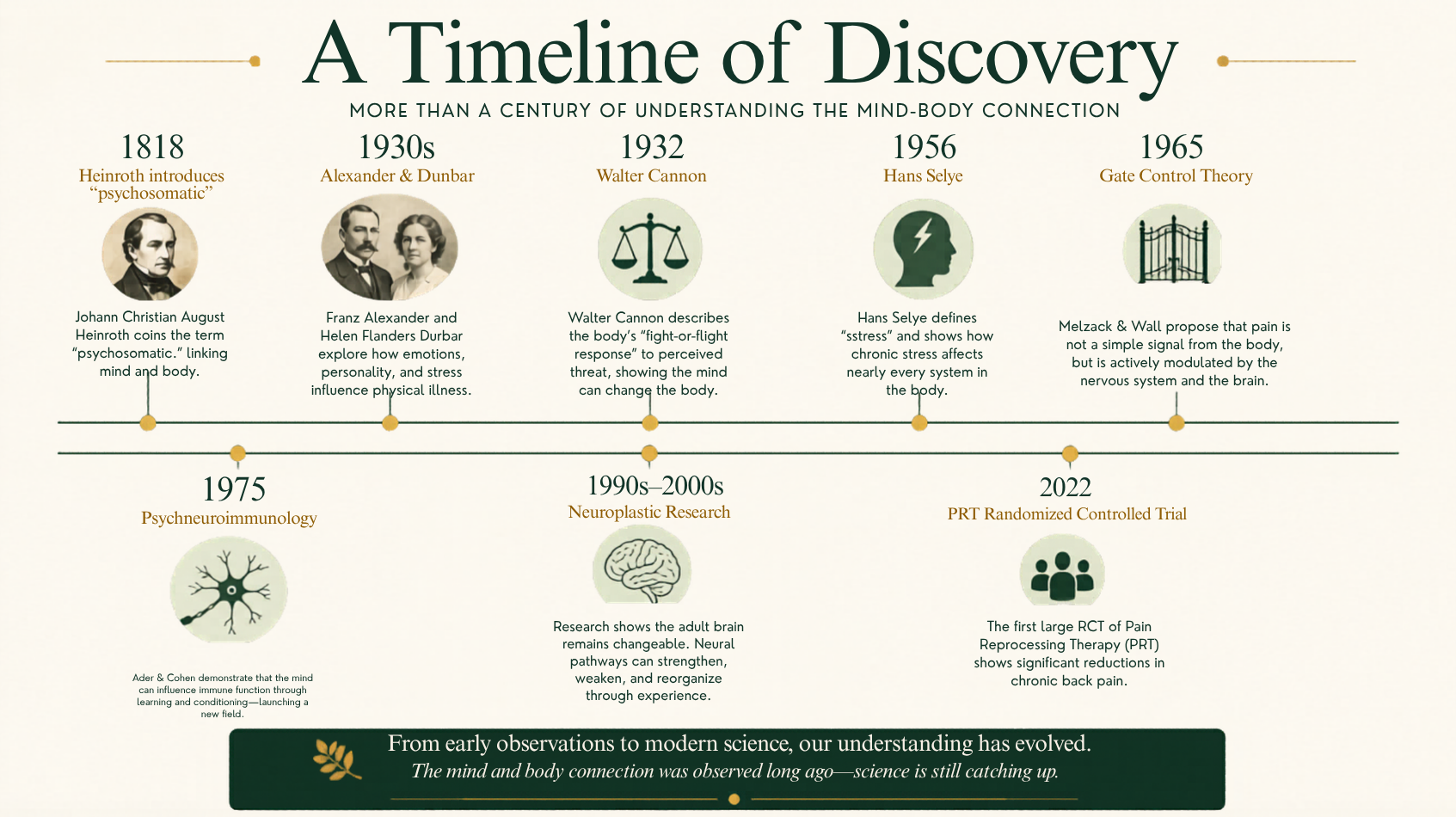
The German physician and psychiatrist Johann Christian August Heinroth (1773–1843) is generally credited with introducing the term in the early nineteenth century.[1]
The idea itself, however, was much older.
More than two thousand years ago, Hippocrates argued that emotional and physical health could not be separated. Throughout history, physicians observed that grief, fear, anxiety, stress, and emotional suffering often produced physical effects.
Anyone who has experienced butterflies before a presentation, lost sleep during a stressful period, or developed muscle tension during a difficult life event has experienced this connection firsthand.
The modern psychosomatic movement began taking shape during the first half of the twentieth century.
One of its most influential figures was Franz Alexander, a physician and psychoanalyst often regarded as one of the founders of psychosomatic medicine.[2]
Alexander proposed that certain physical illnesses might be influenced by specific emotional conflicts. Around the same time, Helen Flanders Dunbar explored possible links between personality patterns and physical disease.[3]
While some of their specific conclusions would later prove too simplistic, their work represented an important shift in thinking.
Rather than dismissing unexplained symptoms, they attempted to understand them.
Their central idea was straightforward:
Human beings cannot be understood as separate mental and physical systems.
The mind affects the body.
The body affects the mind.
Neither operates in isolation.
At the time, this was a remarkably bold position.
What Psychosomatic Medicine Got Right
Looking back today, it is striking how many of the core observations of psychosomatic medicine have stood the test of time.
Researchers repeatedly found that psychological experiences produce measurable biological changes.
One of the most important contributors was Walter Cannon, whose work on the fight-or-flight response demonstrated that perceived danger triggers a coordinated physiological reaction throughout the body.[4]
Heart rate increases.
Stress hormones rise.
Blood flow shifts.
Muscles prepare for action.
The body changes because the brain believes something important is happening.
Later, Hans Selye expanded this understanding through his research on stress.[5]
His work showed that prolonged exposure to stress affects multiple bodily systems and can contribute to long-term health problems.
Over time, evidence continued to accumulate.
Researchers found that stress can influence:
- Pain perception
- Immune function
- Inflammation
- Digestion
- Hormonal regulation
- Cardiovascular health
- Recovery from illness
Today, these observations are no longer controversial.
Few physicians would dispute that chronic stress affects physical health.
The question is no longer whether the mind influences the body.
The question is how.
Where the Early Model Fell Short
For all its strengths, psychosomatic medicine eventually ran into a significant problem.
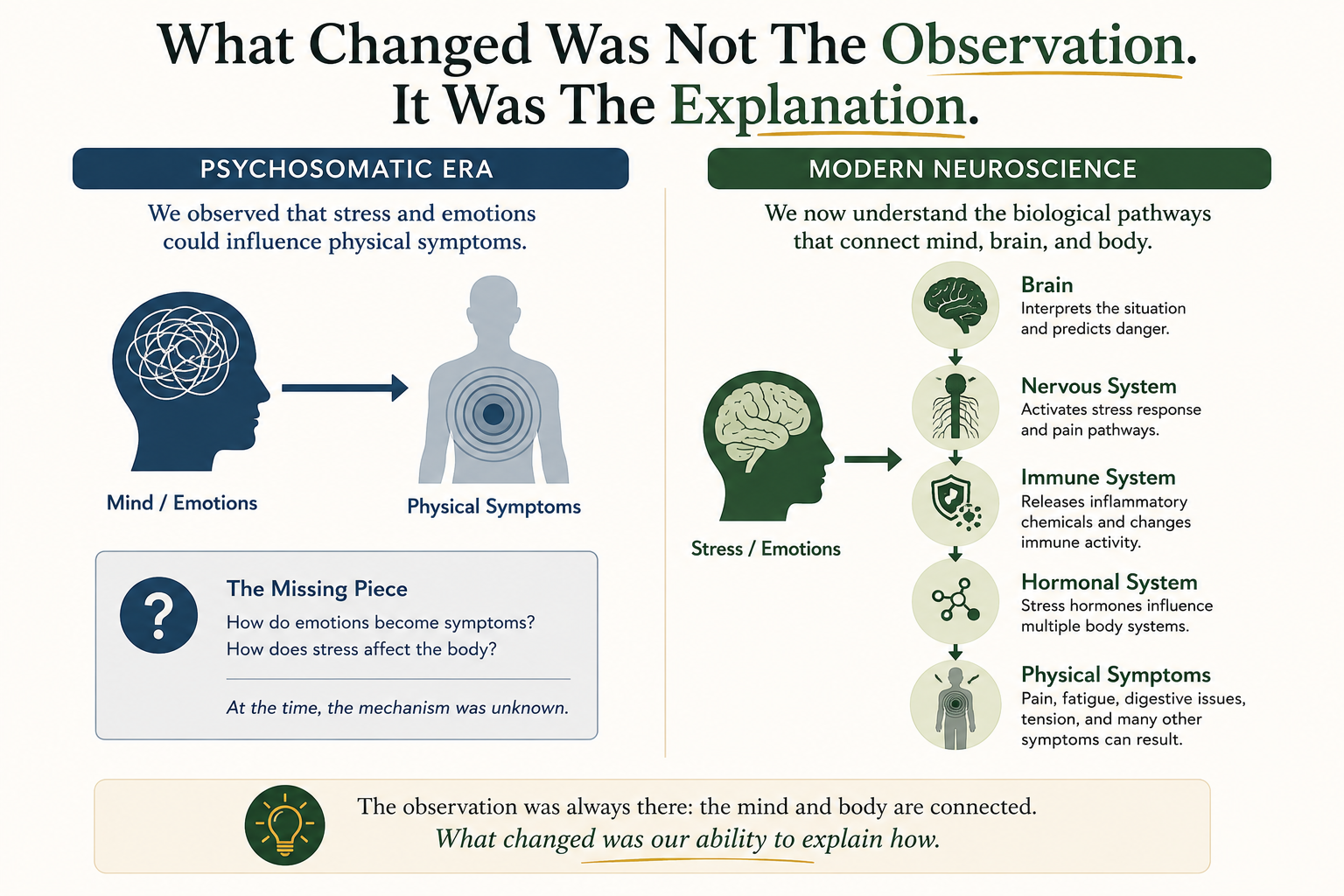
The observations were often correct.
The explanations were often not.
Many early theories relied heavily on concepts such as repressed emotions, unconscious conflicts, and hidden psychological struggles.
While these ideas may have contained elements of truth, they were difficult to test scientifically.
More importantly, they often lacked a clear biological explanation.
How exactly does an emotional experience become a physical symptom?
How does stress become pain?
How does fear become fatigue?
How does emotional strain become digestive distress?
The field struggled to answer these questions.
As a result, many patients received explanations that felt vague or unsatisfying.
Over time, the word psychosomatic itself developed a reputation problem.
Many people stopped hearing:
“Your mind and body are connected.”
and instead heard:
“Your symptoms are not real.”
That was rarely the intended message.
But it became the message many patients received.
The distinction would become critically important in the decades that followed.
The Missing Link: When Neuroscience Entered the Conversation
The transition from psychosomatic medicine to modern neuroplastic approaches did not happen overnight.
It emerged gradually through several scientific developments that, taken together, changed how researchers understood the relationship between the brain and the body.
One important milestone was the emergence of psychoneuroimmunology.
Although the name sounds complicated, the idea is simple.
Researchers began discovering that the nervous system, immune system, and endocrine system constantly communicate with one another.
They are not separate systems working independently.
They function as parts of a larger network.
In the 1970s, researchers Robert Ader and Nicholas Cohen demonstrated that immune responses could be influenced through learning and conditioning.[6]
Their findings helped establish an entirely new field of research.
At roughly the same time, neuroscience itself was undergoing a major transformation.
For much of the twentieth century, scientists believed that the adult brain was largely fixed.
Once developed, it was thought to change very little.
That assumption turned out to be wrong.
Researchers such as Michael Merzenich and Nobel Prize winner Eric Kandel helped demonstrate that the brain remains capable of change throughout life.[7][8]
New neural pathways can form.
Existing pathways can strengthen.
Old pathways can weaken.
The brain continually adapts to experience.
This ability became known as neuroplasticity.
The implications were profound.
If the brain can learn new skills, it can also learn patterns of protection.
If neural circuits become stronger through repetition, then repeated experiences of pain, fear, stress, and vigilance may also leave lasting effects on how the nervous system operates.
For the first time, researchers were beginning to see a possible bridge between psychological experience and physical symptoms.
The question was no longer:
“What psychological conflict is causing this symptom?”
Instead, it became:
“What has the nervous system learned?”
The Discovery That Changed Pain Science
Perhaps nowhere was this shift more important than in the field of chronic pain.
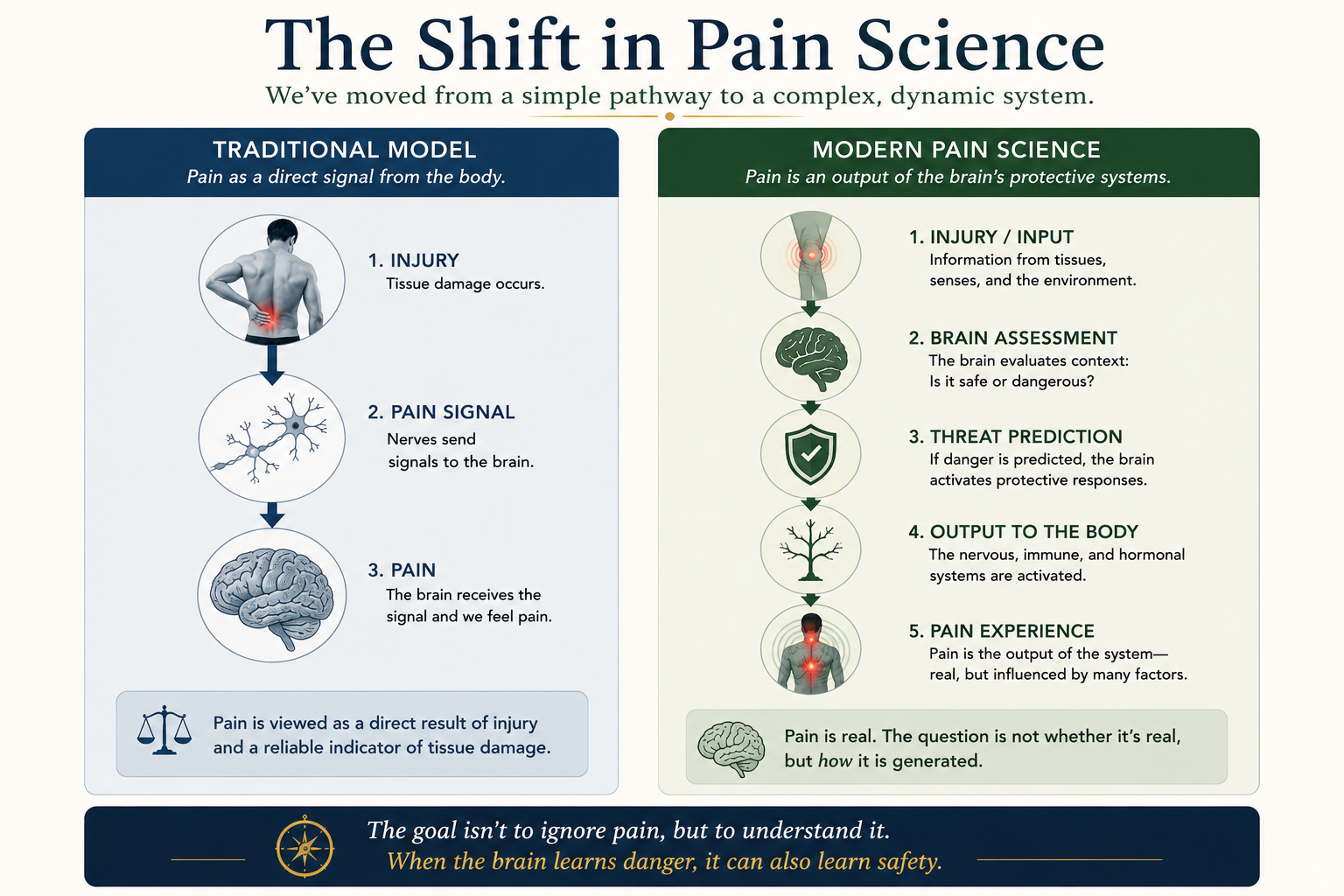
For much of medical history, pain was viewed as a relatively straightforward warning signal.
Injury occurs.
Pain follows.
The injury heals.
Pain disappears.
That model works well for many acute injuries.
It works far less well for chronic pain.
Researchers began noticing something that did not fit the traditional understanding.
Some people experienced severe pain despite relatively minor findings on imaging.
Others had significant structural abnormalities and little or no pain.
Studies repeatedly found disc bulges, arthritis, degenerative changes, and other structural findings in people who had no symptoms at all.
At the same time, many individuals with disabling pain showed findings that did not seem severe enough to explain their suffering.
Something was missing.
A major breakthrough came with the work of Ronald Melzack and Patrick Wall, who proposed the Gate Control Theory of Pain in 1965.[9]
Their theory challenged the idea that pain simply travels from injured tissue to the brain.
Instead, pain appeared to be actively processed and influenced by the nervous system itself.
In the decades that followed, research into central sensitization expanded this understanding further.[10]
Scientists discovered that the nervous system can become increasingly sensitive over time.
In effect, the alarm system can become easier to trigger.
This finding helped explain many observations that had puzzled physicians for decades:
- Pain that persists long after healing
- Symptoms that fluctuate dramatically
- Symptoms that move from one location to another
- Pain levels that exceed what tissue findings would predict
The traditional structural model was no longer sufficient on its own.
Researchers were beginning to see that the brain and nervous system played a much larger role than previously understood.
From Psychosomatic to Neuroplastic
Seen from this historical perspective, modern neuroplastic approaches are not a rejection of psychosomatic medicine.
They are its evolution.
The early psychosomatic pioneers recognized that emotional and psychological experiences somehow influenced physical symptoms.
What they lacked was a clear explanation of how that process occurred.
Modern neuroscience has begun providing that explanation.
Today, many researchers understand chronic symptoms not as evidence of psychological weakness, but as learned patterns within the nervous system.
Symptoms remain real.
Pain remains real.
Fatigue remains real.
Dizziness remains real.
Digestive symptoms remain real.
The difference lies in how they are understood.
Rather than asking only what is happening in the tissues, researchers increasingly ask what the nervous system has learned to predict, expect, and protect against.
In many ways, the central insight has remained unchanged for more than a century.
The mind and body are deeply connected.
What has changed is that science is finally beginning to explain why.
Part II: The Present, the Resistance, and the Future
Pain Reprocessing Therapy and the Next Step in the Story
If the first half of this story is about understanding how symptoms can be influenced by the nervous system, the second half is about what to do with that knowledge.
Over the past two decades, a growing number of researchers and clinicians have explored whether symptoms maintained by learned neural pathways can also be changed by working directly with the brain’s prediction and protection systems.
One of the most visible examples is Pain Reprocessing Therapy (PRT), developed by Alan Gordon and later studied in collaboration with researchers including Yoni Ashar and colleagues.[11]
PRT is built on a relatively simple idea.
If the brain can learn patterns of protection that contribute to chronic pain, then it may also be possible for the brain to learn that certain sensations are safe.
This does not mean ignoring pain.
It does not mean pretending symptoms are not there.
And it certainly does not mean that pain is imaginary.
Rather, it involves helping individuals recognize when the nervous system may be responding to learned danger signals rather than ongoing tissue damage.
The approach combines education, attention training, emotional awareness, and techniques designed to reduce the brain’s perception of threat.
The most widely discussed study of PRT was published in JAMA Psychiatry in 2022.[12] In that randomized controlled trial, participants with chronic back pain experienced substantial reductions in pain, with many reporting little or no pain at follow-up.
The study attracted attention not only because of its results but because it represented the type of evidence mainstream medicine typically looks for when evaluating new treatments.
One study, of course, does not settle a scientific question. Medicine advances through replication, follow-up studies, and continued investigation. Nevertheless, the study marked an important milestone. It suggested that the growing understanding of pain as a learned and changeable brain process could translate into meaningful clinical outcomes.
PRT is not alone in this space.
Related approaches include:
- Emotional Awareness and Expression Therapy (EAET)
- Pain Neuroscience Education (PNE)
- Certain forms of cognitive and behavioral interventions
- Somatic approaches informed by modern neuroscience
- Treatments used for Functional Neurological Disorder (FND)
While these approaches differ in important ways, they share a common assumption:
The nervous system is not fixed.
It can learn.
And what is learned can sometimes be unlearned.
Why Is This Still Controversial?
Given everything discussed so far, a reasonable question remains:
If medicine has known for over a century that the mind and body are connected, and if neuroscience increasingly supports the role of the brain and nervous system in chronic symptoms, why are these approaches still controversial?
The answer lies less in the science itself and more in how medical systems change.
The Success of the Biomedical Model
Modern medicine became one of humanity’s greatest achievements by identifying and treating structural causes of disease.
When someone develops pneumonia, a bacterial infection is found.
When someone breaks a bone, the fracture can be seen.
When a tumor is present, imaging often reveals it.
This approach has saved countless lives.
Its success, however, also shaped how many clinicians think about symptoms.
The basic pattern became:
Find the structural problem.
Treat the structural problem.
Symptoms improve.
For many conditions, that model works beautifully.
For many chronic symptoms, however, the relationship is not so straightforward.
As pain researchers began discovering, symptoms do not always correspond neatly to tissue findings. The more medicine succeeded with structural diseases, the more difficult it became to recognize situations where structural explanations alone might not be sufficient.
Medical Education Moves Slowly
Scientific discoveries and clinical practice do not move at the same speed.
A new finding may appear in research journals today and take years before it becomes part of medical training. Even then, it may take another decade before it becomes routine clinical practice.
Researchers have frequently noted that the gap between scientific discovery and widespread implementation can be measured in years or even decades.[13]
This delay is not unique to mind-body medicine.
It is simply how large systems tend to operate.
Specialization Creates Silos
Modern healthcare is highly specialized.
Orthopedic surgeons focus on bones and joints.
Neurologists focus on the nervous system.
Rheumatologists focus on autoimmune and inflammatory conditions.
Psychologists focus on thoughts, emotions, and behavior.
The challenge is that chronic symptoms often do not respect these boundaries.
The emerging science of pain, stress, neuroplasticity, and symptom generation sits at the intersection of multiple disciplines.
As a result, new ideas sometimes move slowly because no single specialty fully “owns” them.
Financial and Structural Incentives
Most healthcare systems were built around a biomedical model.
Imaging studies, procedures, surgeries, injections, and medications fit naturally into that system.
Education-based interventions, behavioral approaches, and nervous-system-focused treatments often fit less neatly.
This does not require a conspiracy to explain.
It is simply the result of systems evolving around certain assumptions and treatment models.
Changing scientific understanding is difficult.
Changing entire systems is often even harder.
The Language Problem
Perhaps the biggest challenge is communication.
Many patients with chronic symptoms have spent years feeling dismissed.
Some have been told:
“It’s stress.”
“It’s anxiety.”
“Nothing is wrong.”
“It’s all in your head.”
As a result, when they hear that the brain may be involved in generating symptoms, they understandably become skeptical.
The problem is that two very different messages often get confused.
One message says:
“Your symptoms are not real.”
The other says:
“Your symptoms are real, but the nervous system may be playing a larger role than we once understood.”
The first message is dismissive.
The second is an attempt at explanation.
Unfortunately, years of misunderstanding have made it difficult for many people to hear the difference.
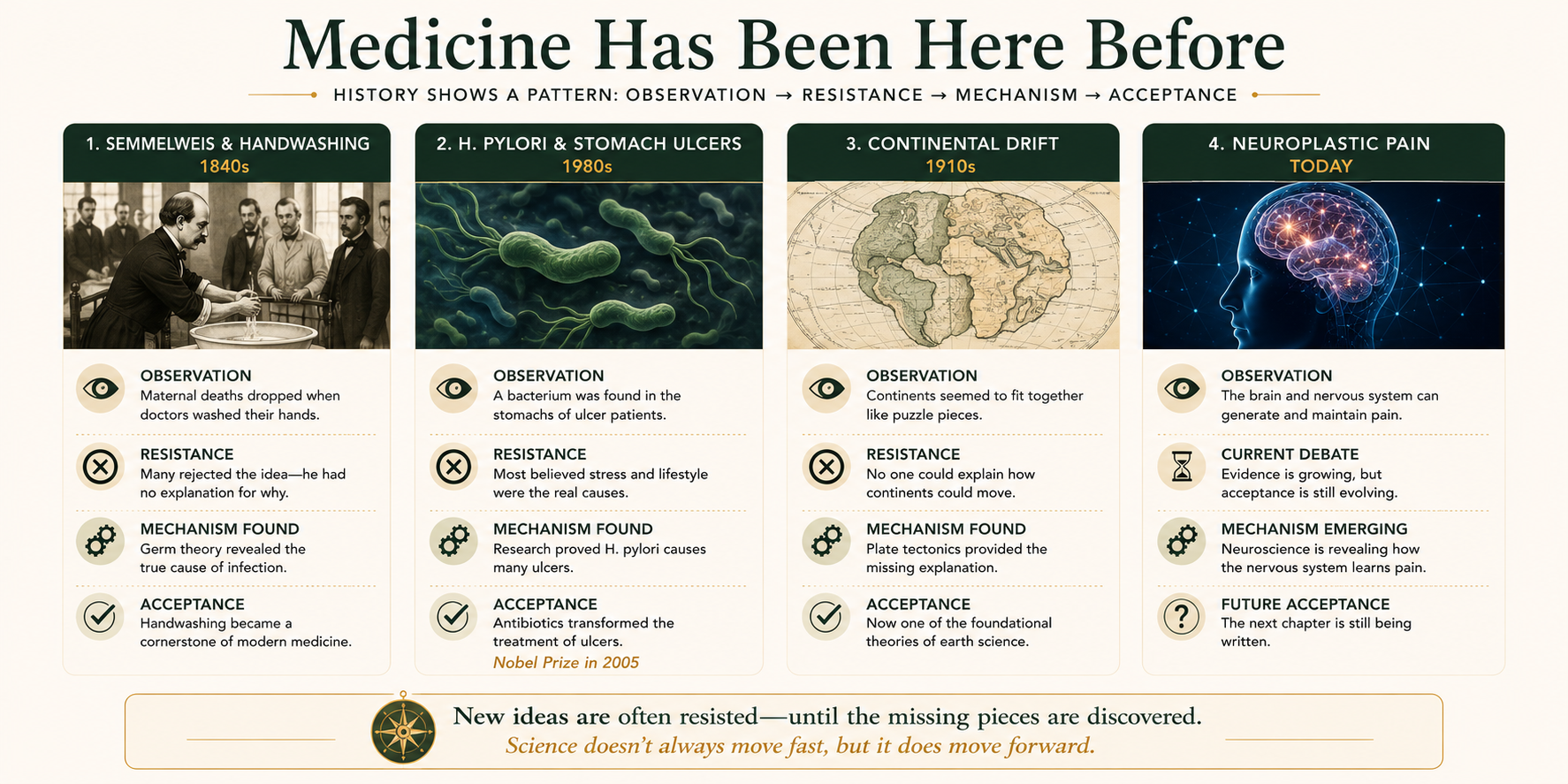
Medicine Has Been Here Before
One of the most useful ways to understand the current situation is to look at history.
Again and again, scientific progress has followed a similar pattern.
Observations appear first.
Acceptance comes much later.
Ignaz Semmelweis and Handwashing
In the 1840s, Hungarian physician Ignaz Semmelweis observed that maternal deaths dropped dramatically when doctors washed their hands before delivering babies.[14]
The evidence was compelling.
The medical community largely rejected it.
Part of the problem was that Semmelweis could not fully explain why handwashing worked.
Germ theory had not yet been established.
Many physicians also struggled with the implication that they themselves might be contributing to patient deaths.
Only years later, through the work of Louis Pasteur and Joseph Lister, did the scientific foundation emerge that explained Semmelweis’s observations.
Helicobacter pylori and Stomach Ulcers
For much of the twentieth century, ulcers were commonly viewed as conditions strongly linked to stress and lifestyle.
In the early 1980s, Barry Marshall and Robin Warren proposed that many ulcers were caused by a bacterium called Helicobacter pylori.[15]
The idea was initially met with skepticism.
Eventually the evidence became overwhelming.
Marshall and Warren were awarded the Nobel Prize in Physiology or Medicine in 2005.
What makes this example especially interesting is that modern medicine eventually concluded that both sides had part of the story.
Bacteria matter.
Stress matters.
Immune function matters.
The final explanation turned out to be more complex than either side originally believed.
Continental Drift
Not all examples come from medicine.
In 1912, Alfred Wegener proposed that the continents had once been joined together and later drifted apart.[16]
Many scientists rejected the idea.
Not because the evidence was weak, but because Wegener could not explain how continents moved.
The observations existed before the mechanism.
Only decades later, after plate tectonics provided the missing explanation, did widespread acceptance follow.
Neuroplasticity Itself
Perhaps the most relevant example is neuroplasticity.
For much of the twentieth century, many scientists believed that the adult brain changed very little after development.
Today, neuroplasticity is one of the most widely accepted principles in neuroscience.
The evidence changed.
The understanding changed.
The textbooks changed.
But it took time.
History rarely moves as quickly as discovery.
What Neuroplastic Medicine Is Not
Whenever a new model gains attention, misunderstandings tend to follow.
Neuroplastic medicine is no exception.
It is important to clarify what these approaches do not claim.
They do not claim that all symptoms are neuroplastic.
They do not claim that structural disease is irrelevant.
They do not suggest avoiding medical evaluation.
They do not deny the importance of biology.
And they do not suggest that every chronic symptom can be solved through mind-body approaches.
Responsible clinicians working in this field generally emphasize the opposite.
Medical evaluation matters.
Structural causes matter.
Inflammation matters.
Infections matter.
Genetics matter.
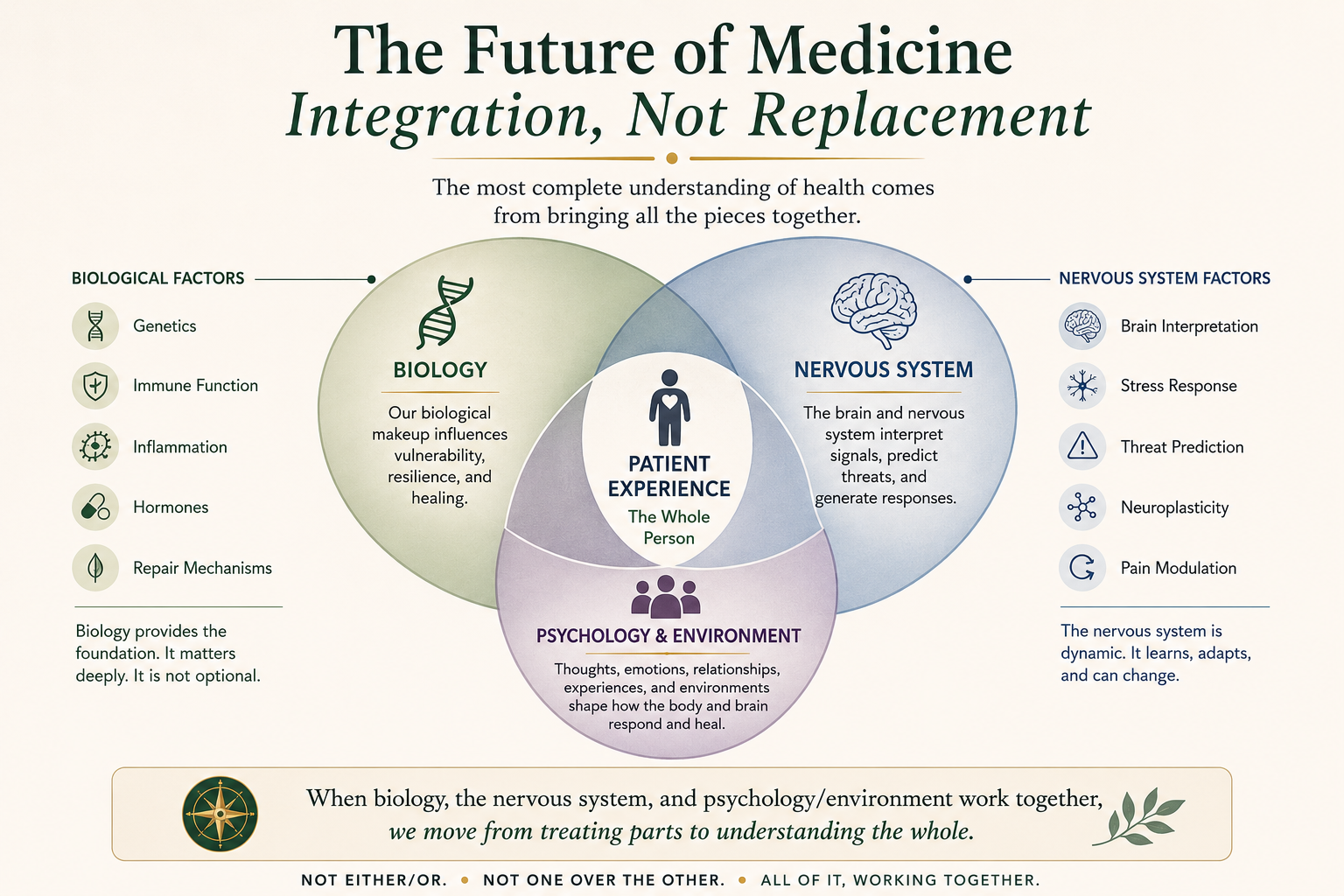
The goal is not replacement.
The goal is integration.
The most likely future is not a choice between biological explanations and neuroplastic explanations.
It is a more complete understanding that recognizes both.
The Outlook: A Slow but Important Shift
If history is any guide, acceptance of neuroplastic and mind-body approaches will probably not arrive all at once.
It will happen gradually.
Pain neuroscience education is already becoming more common in physical therapy and rehabilitation settings.[17]
Research into neuroplastic interventions continues to expand.
The fields of neuroscience, psychology, immunology, and behavioral medicine are becoming increasingly interconnected.
A new generation of clinicians is entering practice with greater exposure to integrated models of health.
Most importantly, patients continue to report outcomes that are difficult to explain through structural models alone.
None of this proves that every claim made within the mind-body field is correct.
Science should remain cautious.
Questions should continue to be asked.
Evidence should continue to be examined.
But the overall direction of the research appears increasingly difficult to ignore.
Conclusion
The story of psychosomatic medicine and neuroplastic healing is often presented as a conflict between old ideas and new ones.
In reality, it is better understood as the gradual development of a single idea.
For more than a century, clinicians have observed that the mind and body are deeply connected.
The early psychosomatic pioneers recognized that emotional and psychological experiences somehow influenced physical health.
What they lacked was the scientific language and technology to explain how.
Over the decades that followed, discoveries in stress physiology, immunology, neuroscience, neuroplasticity, and pain research gradually filled in pieces of the puzzle.
The result is not a rejection of medicine’s past.
It is an extension of it.
The body and brain are not separate systems competing for attention.
They are parts of the same system.
The more science learns about that system, the clearer it becomes that symptoms are often more complex than either purely structural explanations or purely psychological explanations can account for on their own.
The question facing medicine today is no longer whether the brain and body influence one another.
That question was settled long ago.
The question is how quickly healthcare systems, education, and clinical practice will adapt to what a growing body of evidence is revealing about the remarkable learning—and relearning—capacity of the human nervous system.
History suggests that acceptance may take time.
It also suggests that when observations, evidence, and outcomes continue pointing in the same direction, medicine eventually follows.
The body, it seems, often knows first.
The science catches up later.
And the rest of us spend some time in between.
References
[1] Heinroth, J.C.A. (1818). Lehrbuch der Störungen des Seelenlebens.
[2] Alexander, F. (1950). Psychosomatic Medicine: Its Principles and Applications.
[3] Dunbar, H.F. (1935). Emotions and Bodily Changes.
[4] Cannon, W.B. (1932). The Wisdom of the Body.
[5] Selye, H. (1956). The Stress of Life.
[6] Ader, R., & Cohen, N. (1975). Behaviorally Conditioned Immunosuppression. Psychosomatic Medicine, 37(4), 333–340.
[7] Merzenich, M.M. (2013). Soft-Wired: How the New Science of Brain Plasticity Can Change Your Life.
[8] Kandel, E.R. (2006). In Search of Memory.
[9] Melzack, R., & Wall, P.D. (1965). Pain Mechanisms: A New Theory. Science, 150(3699), 971–979.
[10] Woolf, C.J. (2011). Central Sensitization: Implications for the Diagnosis and Treatment of Pain. Pain, 152(Suppl 3), S2–S15.
[11] Gordon, A. (2021). The Way Out.
[12] Ashar, Y.K., Gordon, A., Schubiner, H., et al. (2022). Effect of Pain Reprocessing Therapy vs Placebo and Usual Care for Patients With Chronic Back Pain. JAMA Psychiatry, 79(1), 13–23.
[13] Morris, Z.S., Wooding, S., & Grant, J. (2011). The Answer Is 17 Years, What Is the Question? Journal of the Royal Society of Medicine, 104(12), 510–520.
[14] Semmelweis, I. (1861). The Etiology, Concept, and Prophylaxis of Childbed Fever.
[15] Marshall, B.J., & Warren, J.R. (1984). Unidentified Curved Bacilli in the Stomach of Patients with Gastritis and Peptic Ulceration. The Lancet, 323(8390), 1311–1315.
[16] Wegener, A. (1915). The Origin of Continents and Oceans.
[17] Moseley, G.L., & Butler, D.S. (2017). Explain Pain.



